|
|
♦ PSI Institute Phone: 027 657 2106 E-mail: jlightstone-at-gmail.com RELATIONSHIP AND COUPLES THERAPY ♦ PSI Institute 254 Lincoln Road Henderson Auckland New Zealand ♦ Phone: +64 (0)27 657 2106 ♦
|
"Click
here for more Blossom Fuller"
© by Judy Lightstone, 2012
 Let’s
start by defining compulsive eating as any eating out of relation to physiological
hunger and satiation. This means that anytime one eats for reasons
other than hunger or bringing hunger to satiation, we say that eating was
compulsive in nature. Which is to say we all eat compulsively at
times (i.e. for reasons other than physiological hunger). Let’s
start by defining compulsive eating as any eating out of relation to physiological
hunger and satiation. This means that anytime one eats for reasons
other than hunger or bringing hunger to satiation, we say that eating was
compulsive in nature. Which is to say we all eat compulsively at
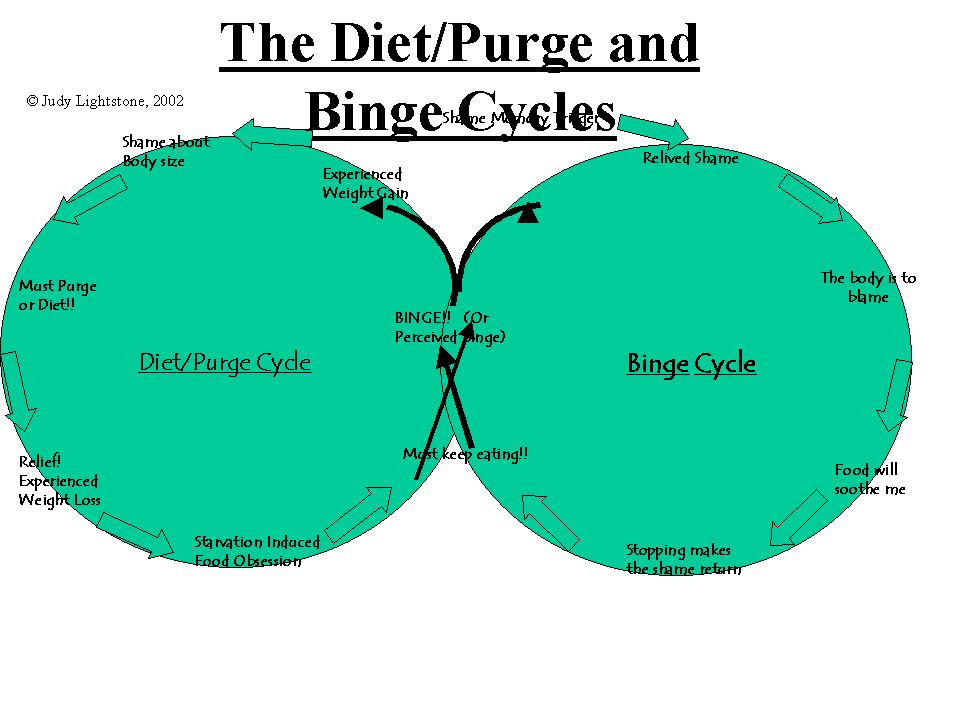
times (i.e. for reasons other than physiological hunger).People with eating problems, however, eat compulsively consistently and feel terrible shame about both the behaviour and the effects of the behaviour (perceived or real) on their body size. In fact, each compulsive eating episode tends to be accompanied by a great deal of shame, as shown in the cycles below. Indeed it could be said that shame is the main ingredient that turns a "normal" experience of compulsive eating into a repetitive anguished pattern. In my work with people with eating disorders, I listen to them carefully as they describe their eating in detail to me. Below is a common pattern I have distilled from underneath the many stories I have heard.
As you see above, the binge (or perceived binge) is initially triggered by an event or thought that may also be associated to an earlier less conscious experience. The earlier experience may have included a great deal of shame. That experience is then transferred to feelings of body shame, and self-critical thoughts. At this point the person reaches for food to help salve the pain. The shaming thoughts are then redirected onto the eating behaviour, which puts the eating in a paradoxical role. While it is soothing the person, it also acts as a scapegoat for the bad feelings that triggered the binge to begin with. The eating behaviour, and the soothing it brings, then becomes the enemy. The person then believes “I feel bad because I am eating” rather than “ I felt bad and so I ate”, because they no longer remember what made them reach for the food in the first place. The person then has to keep eating because
they still feel bad, and so they start to feel bad because they can’t stop
eating.
Example: JL: What do you think made you go for the
Oreos at 2PM yesterday?
Pt: I had a huge binge last night.
This approach goes against so many socially imposed beliefs that it is sometimes difficult to follow. However, most realize that it makes sense, once they are more in tuned with their patterns of hunger and satiation. There are even people in OA groups that are now defining abstinence in terms of only eating with hunger and satiation, which is a much more natural definition of abstaining from compulsive eating, in my opinion, than sticking to a low calorie food plan or avoiding "addictive" foods or food groups. According to the World Health Organization, an adult female requires 2,000-2,500 calories per day (depending on degree of activity). Less than that is, by definition, substandard, and your body will fight hard to get and keep those calories. Most restrictive food plans (as they are often called now that dieting has gotten a bad rep) attempt to keep your caloric intake below these basic requirements, and so, are bound to rebound eventually. The dieter then blames him/herself and feels ashamed, fuelling the die/binge cycles to continue. If you would like to form a support or therapy group to work on your eating problems, click here |
|
254 Lincoln Road, Henderson, Auckland, New Zealand. E-mail: jlightstone-at-gmail.com Phone +64 (0)27 657 2106HOME PSYCHOTHERAPY RELATIONSHIP THERAPY LIST OF ARTICLES ABOUT JUDY CONTACT MEPROFESSIONAL DEVELOPMENT LOCAL SUPERVISION ONLINE & DISTANCE LEARNING |
 Auckland PSITM
Auckland PSITM